



By mobilizing around the dire need to protect oneself and community to reduce the risk associated with injecting drug use during the HIV/AIDs epidemic, “harm reduction” was born. There was a keen awareness that the government, care providers, and society didn’t care about the injection drug user population (or LGBTQ+ folks). Those who were at the highest risk of HIV/AIDS, were left by the state to die. Impacted people mobilized on the ground to teach each other how to protect themselves and distribute any kind of resources attainable. They grew to actively urge government entities, public health officials, and the average person to consider, implement, and fund a variety of models for approaching drugs that aren’t solely grounded in abstinence-based and prohibitionist values. It was a radical, activist movement when people who use drugs (PWUD) started to demand that governing bodies see PWUD as people who were not only not being served by existing conditions, but actively harmed.
The origins of harm reduction spawned from a radical social movement that’s more than the set of strategies and resources (like opioid overdose reversal drug distribution and syringe exchange). Harm reduction challenges how society and policymakers conceptualize certain drugs and populations of people using those drugs.
While groups like the Young Lords Party and Black Panther Party were already organizing community-based harm reduction health-motivated direct actions and community support in the 1970s, it wasn’t formally recognized as a public health model until the 1980s. In the early 80s a harm reduction model was implemented in the Netherlands as harmful drug use and the comorbidity with HIV/AIDS was becoming more prevalent (notably, the demographic of PWUD widened). The existing prohibitionist model was not structurally sustainable and became unpopular with the public. To combat the growing health concerns, the Netherlands expanded (the already existing) needle exchange and distribution programs.
In the United States and Canada, organizers, advocates, communities, and renegade care-providers were already opposing legal restrictions on drugs and the criminalization, marginalization, and oppression of PWUD prior to the 80s (and before the “War on Drugs” was formally declared by Richard Nixon). When the HIV/AIDS epidemic worsened and started to impact more people, grassroots harm reduction communities started to organize with LGBTQ+ groups to save each other’s lives. If the government wasn’t going to help, then the people most impacted would help themselves.
Harm reduction started to gain traction out of necessity. The official terming of this approach can be traced to Russel Newcombe, a research psychologist, who published an article using “harm reduction” to describe Allan Parry’s work with a risk reduction clinical syringe exchange service based on the Dutch programs in Liverpool in 1986 (but please note that people were already practicing risk reduction education and techniques prior to this).
Communities were organizing to save themselves and their peers by teaching people who inject drugs to clean their needles with bleach and resist sharing when they could. Meanwhile, the local and federal government (which had a different socio-political landscape and history of strict prohibition and criminalization of Black and working class PWUD than the Netherlands) stumbled to find the legal support to implement needle exchange programs. Despite the plethora of evidence from scientific studies proving the multitude of social, societal, and health benefits that syringe exchanges and safe consumption sites offer, opposition to needle programs made implementation difficult. Driven primarily by state and federal legislature, drug-user stigma, misinformation campaigns, and existing punitive systems against PWUD — needle distribution has been fragmented from the start and is still divided as of the time of writing.
Note that these needle exchange programs offer more than sterile needles and syringes. These community-based programs can also provide referrals to substance use disorder treatment programs and other social and mental health care services, health screenings, 1-1 peer support, treatment for hepatitis and HIV, education about overdose prevention and safer injection practices, vaccinations, and beyond (services vary by site). According to many studies, major health organizations, and the Center for Disease Control and Prevention (CDC), these programs can help people reduce the harm of their drug use, stop using drugs, reduce infections, reduce drug overdoses, are cost effective and do not lead to more crime and/or drugs use.
Safe consumption sites (SCS or harm reduction centers) offer another technique and space for drug users. In July 2021, Rhode Island was the first state in the United States to legally authorize a two-year pilot drug consumption space, harm reduction center, and program. In November of 2021, New York City authorized two supervised injection sites in Manhattan that have already been saving hundreds of lives (writing in July 2022). DecrimPovertyDC is Washington, DC’s coalition to bring a overdose prevention site (and other harm reduction measures) to the District.
Despite decades of evidence, stigma and legal barriers still restrict access to the creation, funding, and utilization of these needle exchanges and safe consumptions sites in the United States. From the beginning, people running needle exchange services operated under illegal conditions via community organizing. Exchanges eventually gained funding through private and local means. In 1989, Congress voted that Federal money would not support needle programs and a decade later, despite plenty of evidence depicting the positive effects of these programs, the Clinton administration refused to lift the ban as they succumbed to drug fearmongering. Needle exchange and federal support has flipped a couple times under the Obama administration and the ban was partially lifted in 2016. While it was still federal law to prohibit the use of federal funds to purchase sterile needles or syringes, the funds could be used to pay for other aspects of needle exchange programs. In July 2021, the House Appropriations Committee approved a funding bill for 2022 that will allocate five times more money to harm reduction resources than the previous year that will also expand syringe service programs. It’s vital to understand that a presidential administration or government support of “harm reduction” doesn’t always align with on-the-ground and traditional understanding of the movement, philosophies, and implementations.
[For more information on needle exchange programs see: https://www.aclu.org/fact-sheet/needle-exchange-programs-promote-public-safety]
Practices and programs carried out by harm reductionists exceed needle exchange programs and safe consumption sites. Again, it is rooted in bottom-up community led efforts to address any gaps and structures of harm that governments and medical providers have caused and/or neglected. It was born from the struggle against ineffective, violent, punitive, moral models of “addiction”; it rose from health injustices and disparities. And it’s not just for people who use drugs. These principles, commitments, advocacy, activism, and services can be applied to unhoused people, sex workers, sex, and many other behaviors that impact people from every walk of life.



")

The elimination of criminal penalties for drug-related possession, consumption, and sale has been a particularly hot topic during the 2020 general election. The harm reductionist stance recognizes that when drugs are criminalized that specific populations are being criminalized. The criminalization of people who use drugs was directly challenged on a massive level when voters in Oregon passed decriminalization of all drugs (measure 110) and voters in New Jersey, Montana, Mississippi, Arizona, and South Dakota (medical use) legalized marijuana. These new measures indicate a shifting conceptualization of PWUD and treatment in political, economic, public health, and mainstream public opinions.
Measure 110 spearheaded by Drug Policy Action, opposes and seeks to undo the decades of tough on crime policies and drug war violence that have harmed so many people — specifically Black and Brown communities. Cannabis tax revenue and funding saved from decreasing drug policing, jailing, and imprisonment will now go to treatment, other public health services, and social resources (like housing and harm reduction!) without raising taxes.
As the Drug Policy Alliance mentions, there are projections that this shift will result in a 95% decrease in racial disparities in drug arrests.
Just like needle exchanges and MAT, decriminalization does not encourage more drug use or crime — it reframes how drug is conceptualized and treated by meaningfully addressing the health and autonomy of the person using (rather than just violating, incarcerating, or otherwise harming them — or in many ways, letting them die).


Since 1971 when Richard Nixon declared the “War on Drugs”, implemented tough drug policies, expanded drug agencies (which all expanded under Ronald Reagan’s anti-drug campaigns) there are ten times more people behind bars for a drug law violation. This was not to punish drug use – it was to punish social movements (anti-war) and people (Black Americans) and that intel is recorded.
Policies related to the War on Drugs have drastically increased the number of people arrested, convicted, and incarcerated for drug-related crime. At the federal level, “people incarcerated on a drug conviction make up nearly half the prison population. At the state level, the number of people in prison for drug offenses has increased nine fold since 1980, although it has recently started to decline. Most are not high-level actors in the drug trade, and most have no prior criminal record for violent offenses” according to the Sentencing Project. Data from 2014 indicates that incarceration is not an effective drug control and prevention strategy – even in strictly economic terms there’s a high cost with low return. Not to mention all the lives, families, and communities that incarceration has disproportionately targeted, impacted, and disrupted.
The over-policing and over-incarceration of PWUD have led to 65% of the prison population with an active substance use disorder (SUD) and another 20% who do not meet the official SUD criteria but were under the influence of drugs or alcohol at the time of their crime.
Drug policy problematically targets and punishes users and sellers (which is a blurry, ineffective distinction) rather than addressing health or the conditions that produce drug use while disproportionately targeting and impacting Black and Latino people.
The lack of efficiency in decreasing crime and/or drug use with punitive measures proves that this system is (unsurprisingly) ineffective, but also focused on fueling the prison industrial complex, punishing rather than rehabilitating, and creating/maintaining a social order rather than combatting crime or helping PWUD. Decriminalization is vital to racial justice. Criminalization does not, and has never, improved lives at large — it ruins lives. Including the violence of policing, arrest, and incarceration, being criminalized marks people which “creates barriers that can trap people in a cycle of poverty and discrimination and lead to higher rates of chronic health issues and substance use disorders” according to the Drug Policy Alliance. So, the drug war and criminalization exacerbate — rather than alleviate — the conditions that fuel harmful substance use (like insufficient housing, poverty, resource poverty, lack of social systems, racism, etc.).
As Johnny Bailey, community outreach coordinator at HIPS, says about incarceration, “when has the legal system actually helped addicts? I know whenever people are like, ‘drugs will ruin your life’, a quarter of that, minimum, is the legal part of them ruining your life. And when people go in, you go in for a 10-year, a 10-year bit or something, and you’re not coming out to the ability to get a decent job, right? And in that 10 years, you could have done all sorts of things that are going to turn you around. No matter what you turn around in prison, you’re probably coming out to a world that’s hard.”
[More on understanding and dismantling the drug war can be found on Drug Policy Alliance website.]
Decriminalization of all drugs in Oregon, the growing number of states with marijuana decriminalization, more safe consumptions sites, and the change in federal funding that may now be used to purchase fentanyl test strips (FTS) indicate promising shifts in popular opinion about the societal understanding of drugs, mitigating harm, and shift towards health services rather than criminalization. As of October 2021, HIPS and the Drug Policy Alliance are spearheading a campaign, #DecrimPovertyDC with a coalition of over 40+ groups to “decriminalize drug use and possession, and instead address collateral consequences of drug convictions and invest in evidence-based public health approaches that dignify and support people who use drugs” according to the campaigns website.


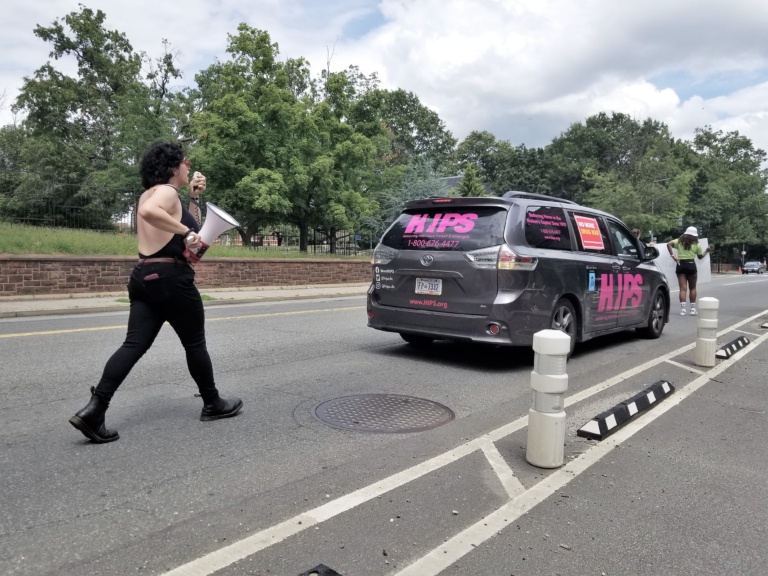
 Formed in 1993 by community representatives, HIPS (Honoring Individual Power & Strength) initially mobilized around youth sex worker outreach and counseling in the District. They have since expanded programming to address to following: HIV/AIDS education, testing, and resources; peer education programming; drug use safety, education, and substance use treatment; overdose prevention services; syringe exchange; programs specifically for LGBT+ sex workers and safety; counseling; educational and training services; housing services; virtual medical appointments; and more.
Formed in 1993 by community representatives, HIPS (Honoring Individual Power & Strength) initially mobilized around youth sex worker outreach and counseling in the District. They have since expanded programming to address to following: HIV/AIDS education, testing, and resources; peer education programming; drug use safety, education, and substance use treatment; overdose prevention services; syringe exchange; programs specifically for LGBT+ sex workers and safety; counseling; educational and training services; housing services; virtual medical appointments; and more.
HIPS’ brick and mortar drop-in center is located on 906 H street NE. They also provide mobile supply and medical services on their outreach van and a 24-hour crisis hotline. As mentioned by outreach staff, HIPS develops as the community needs them. If there is a demand or a need, they do their best to add it under their umbrella (demonstrating their commitment to the communities).
In addition to providing these vital resources, services, and training to sex workers, the LGBTQ+ community, and PWUD in the District, HIPS is active in policy and advocating for the rights of drug users, sex workers, and trans people. In 2020 HIPS and the Drug Policy Alliance jointly submitted a letter to DC Council for the removal of criminal penalties for the possession or distribution of what’s been deemed “drug paraphernalia”. In November, the Opioid Overdose Treatment and Prevention Omnibus Amendment Act of 2020 was unanimously advanced (although it still awaits to be effective as law). This decriminalization is a strong step forward for public health, harm reduction services, PWUD, and racial justice in the district.
On the tail end of this win, in 2021, the Drug Policy Alliance and HIPS organized a coalition of 40+ organizations and teamed up again to launch the campaign #DecrimPovertyDC. The mission is, “through ongoing advocacy, we aim to replace carceral systems with harm reduction-oriented systems of care that promote the dignity, autonomy, and health of people who use drugs, sex workers, and other criminalized populations.” Learn more about the movement and get involved here!
Amidst the worldwide pandemic in 2020 that exacerbated existing inequalities and health concerns, the clinical services team cured 154 people diagnosed with Hepatitis-C, started to provide gender affirming hormone therapy, and distributed 550,000 sterile syringes (272,000 more than 2019), and distributed 12,459 naloxone kits (more than doubled from 2019).
[You can find all of HIPS policy recommendations here.]










{kind=link}
{kind=link}
{kind=link}

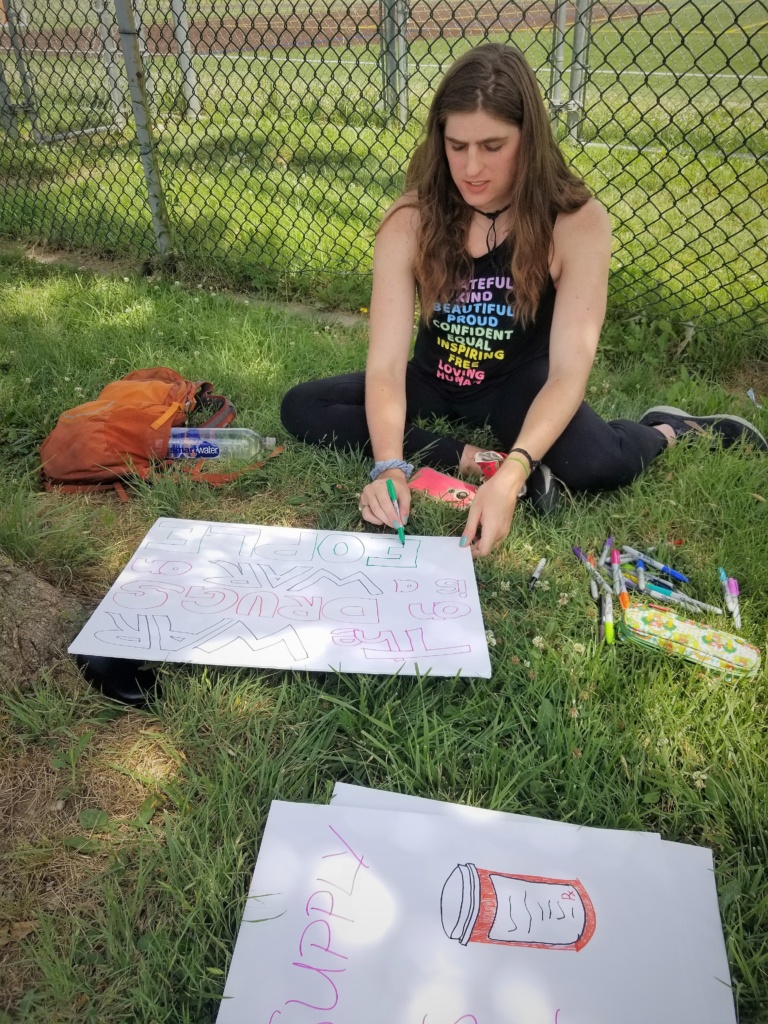
This time HIPS and the Humanities Truck collaborated with DC Ward 1 Mutual Aid, Revise Inc., ACLU of DC, and Stop Police Terror Project DC at Temperance Alley where we tabled, shared community info, ate Ben’s Chili Bowl, told stories of recovery, gathered for overdose reversal training and resource distribution, and had plenty of fun to fill our cups.
Temperance Alley is an abandoned community garden behind 1909 13th street. Mutual aid and local groups have reclaimed this space, this space that is technically owned by developers who will erect a 105-foot hotel and apartment complex. These plans are not until 2023 so in the meantime community members are using the space as a park, community garden, and outdoor classroom “designed by neighbors, for neighbors” where they do park beautification, meditations, storytelling, lawn games, yoga, and so much more.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
